News this past week has been full of information about COVID-19 vaccines and the antibody responses of people who have become sick. While some sources take care to explain the information, others are hyping up whatever headline they think will grab more clicks from their viewers. Because of the chaos and conflicting information, I will be diving into the immune system and what that means for the COVID-19 response.
The Immune System – A Summary
We get sick when some foreign entity such as a virus, bacteria, or parasite enters our bodies. When these foreign entities seek to use our bodies to establish themselves, they are recognized as pathogens and the immune system activates to throw out the hostile invaders. There are two types of immunity, an innate immunity which recognizes patterns common to pathogens and an adaptive immunity which recognizes individual pathogens through trial and error. By combining these two systems we have a powerful ability to identify and eliminate pathogens. But alas, as in all warfare it’s a constantly changing field and pathogens are constantly trying to evade the immune system by changing too.
Everything living is in a constant state of flux driven by mutations. Mutations themselves are not good or bad, they are just the engine of change in biology. While we generally recognize mutations as something bad, there are thousands of mutations that occur and cause no change at all. Sometimes mutations occur that either by themselves or combined with other mutations allow for drastic changes in function.
Your immune system can identify what belongs, what doesn’t belong, and when something is wrong. It’s easiest to think of the immune system as your body’s security force, with information on how to identify everything that doesn’t belong.
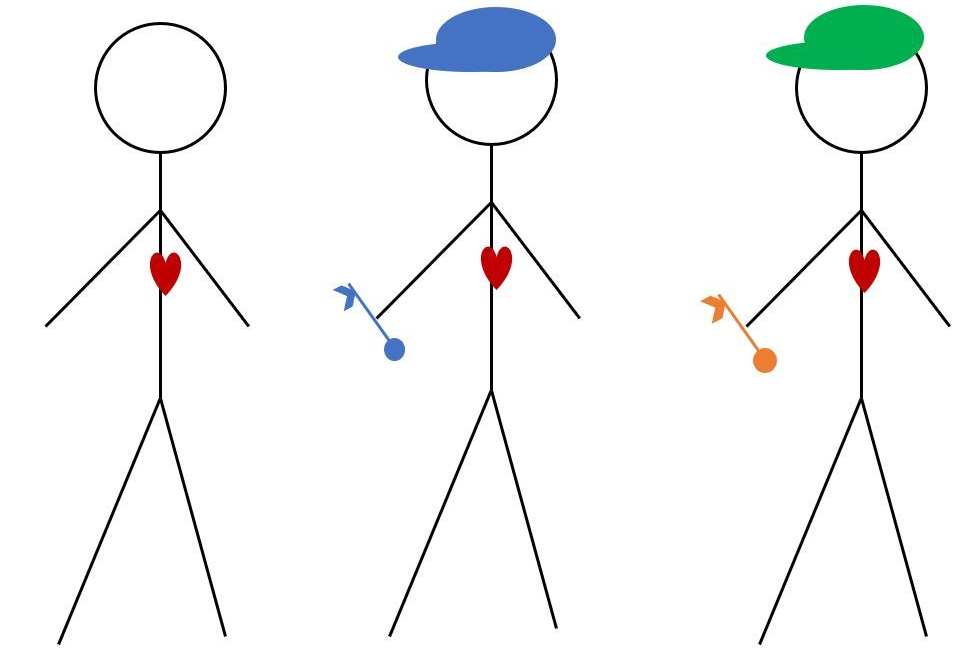
The adaptive immune system is first taught to recognize a healthy cell and all of it’s parts, so that it can then identify what isn’t normal. In my stick figure drawing the immune cells have three ways to identify a pathogen, the hats, the keys, and by seeing what’s in their hearts which represent their genetic information. Hats and keys are external markers that are easily detected by the immune system, these are meant to be parallels to surface proteins which can be unique to pathogens and not present on normal cells. If the immune system is trained to recognize the presence of a hat or a key as the marker of a pathogen there will be a much broader response than if the immune system is trained to only recognize blue hats or gold keys.
After exposure to a new pathogen the adaptive immune system’s B Cells develop antibodies that can attach to parts of the pathogen and flag them for removal. This is much the same as identifying someone wearing a green hat as a person of interest as antibodies flag to superficial features of a pathogen and alert the immune system to react. A neutralizing antibody is one that can stop the pathogen from functioning in some form or fashion. For COVID-19 neutralizing antibodies have been classified as those that bind to the spike protein in such a way that it prohibits SARS-CoV-2 from entering the cell, represented in the cartoon by the key. So while flagging the viruses’ green hat helps find them, flagging the viruses’ key actually stops them from using that key to get into cells.
T cells are the means by which the immune system attacks pathogens. This is a type of cell that is critical to the immune response. When cells are infected with a virus their functions are taken over and become slaves to the virus. T cells are trained to fight against specific pathogens and can identify and eliminate infected cells over and over again.

With the innate immune response and the adaptive immune response, our bodies have a huge capacity to fight off and even prevent infection from pathogens. While the innate immune system is always ready to go, the adaptive immune system needs exposure to a disease before it is fully capable of mounting a response, but once that exposure occurs the adaptive immune system is ready for the fight.
Herd Immunity
When a large proportion of a population does not spread a disease to anyone who is vulnerable, that group is said to have attained herd immunity. The group, or herd, works together to protect the vulnerable people who either cannot be vaccinated or would have severe problems if they ever got sick. While this works for many diseases, there is mounting evidence that depending on herd immunity will not be a valid way to manage COVID-19.
The percent of people needed to establish herd immunity is based on the disease’s R0, a value that shows how many people one sick person will go on to infect, and how many people need to be immune to the disease to bring the R0 to 0. For most diseases the percent of people immune to the disease required to provide herd immunity is over 60%. Without a vaccine, that means at least 60% of the people in a given community, city, state, or country, would have to get sick and develop a neutralizing antibody response before we can start seeing the virus slow down without other measures in place. [link]
The United States has a population of 328.2 million people; as of July 26th, 20202 there have been 4.2 million known cases in the US and 146 thousand COVID-19 related deaths. [link] If we use the known case and death numbers and extrapolate the numbers we would see with 60% of people in the US getting sick, there would be 196.9 million cases and 6.8 million deaths. At this point, the cost in deaths is too high to rely on herd immunity alone. To make this plan even worse, there’s emerging data that antibodies may not last more than a few months.
COVID-19 Antibody Response
While antibody testing has been available since early 2020, there were initial problems with the quality of tests and how well they were actually able to detect antibodies specific against SARS-CoV-2. [link, link] Since June there has been more control by the FDA on available COVID-19 antibody tests that are able to detect the presence of antibodies specific against SARS-CoV-2 rather than other corona viruses. With these more precise antibody measurements, scientists have been able to track how many people have specific antibody responses and how long those antibodies are present after people recover.
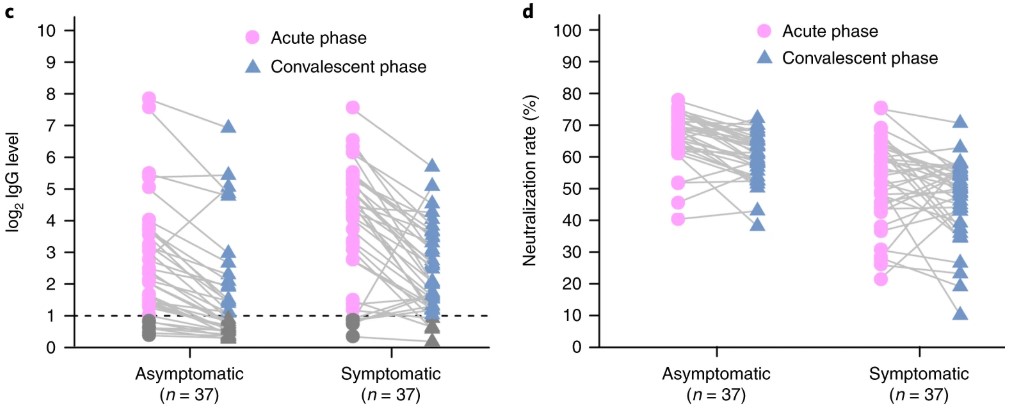
One study published at the end of June followed a total of 74 people, 37 asymptomatic and 37 symptomatic, who tested positive for SARS-CoV-2. This study comes from Wuhan, the original site of the outbreak, where anyone who tested positive were moved to a hospital for monitoring and to minimize spread of the virus. While all of the people involved in the study had similar amounts of virus detected, the symptomatic patients were found to have higher antibody responses. The patients had their antibody responses retested 8 weeks after being released from the hospital. Patients who were symptomatic had a stronger antibody response but a majority of all patients showed weaker antibody responses compared to their results during SARS-CoV-2 infection. [link]
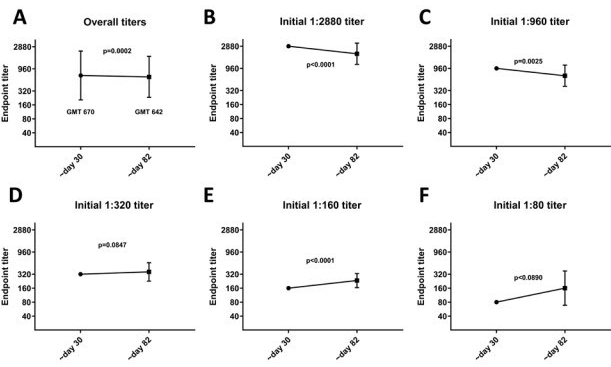
Two more studies have come out in July, one with a 34 person study where everyone was known to be positive and a second with 19,860 people who were established to have a COVID-19 antibody response. [link, link] The smaller study matches the pattern of the initial study where antibody response wanes over time while the larger study shows little change in titres after a nearly 3 month follow up. It’s no surprise to see studies in conflict with each other this early into what is essentially a new field, as we are just now trying to figure out what’s going on and a lot of data can be flawed.
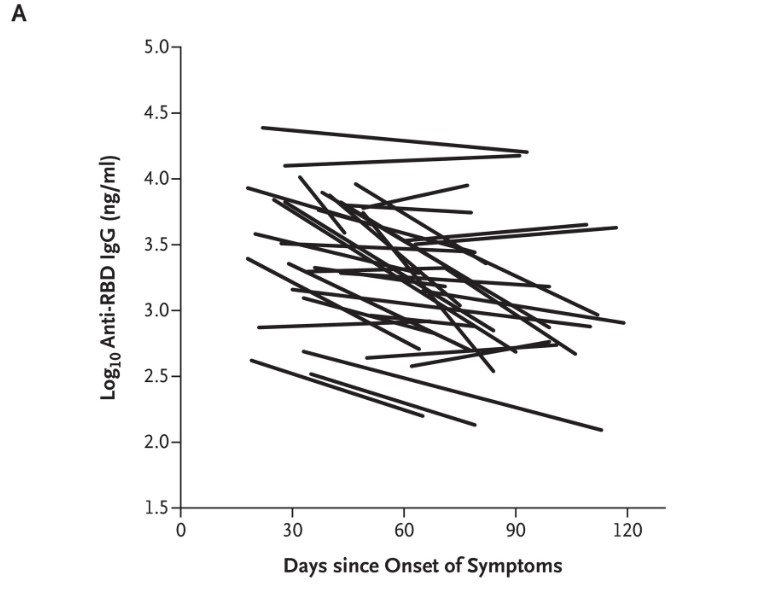
Both studies look out to three months after onset of symptoms and do not show what the antibody response was like while the person was sick. The smaller study establishes that the antibody half life for the patients they followed was 26-60 days, meaning that once that time period has elapsed then the number of antibodies present was half. The larger study looked at a large number of people, over 50,000, who claimed to have experienced COVID-19 and while nearly 20,000 tested positive for the initial antibody response, at least 3 days after experiencing symptoms, only 121 people were included in the follow up study to check for duration of their response. This study most likely missed some of the weakest antibody responses and possibly biased their data towards stronger responses that were easier to detect. While the 121 duration participants did come from a variety of response intensities, there was a wide variety of responses which caused large ranges of errors that shows the variation within the study’s participants.
All told, there has been no definitive study of the duration of antibody responses for COVID-19 as the test to measure the response was only created in recent months. For the short term we know that while some people may have antibody responses that can last for a few months, there is clear data that people with mild symptoms can lose their response in the same time frame.
Because of the possibility for antibodies to disappear, some people have become worried about if a vaccine will actually be possible for COVID-19. The good news is that vaccines don’t work the same way infections do and there’s still hope vaccines can generate the herd immunity necessary for us to return to normal activities.
Hope through Vaccines
The reason vaccines may still work is because scientists are able to design vaccines to have just the right immune response. Rather than showing an entire virus to the body a vaccine can display just a part, such as the key in the pathogen cartoon, that is just what the body needs to develop the proper neutralizing antibodies. Additionally, vaccines are able to be given multiple times to boost the immune response and improve the antibody titers to protective levels. Normally with a disease we know what to target and how much antibody is necessary to protect against future infection but with SARS-CoV-2 it’s just too early to know. Hopefully soon we will begin to see information about the amount of antibodies needed to protect people from infection as there are studies looking into that at this very moment.
While that work is currently ongoing, scientists are doing their best to elicit the strongest possible immune response by measuring not just antibodies but also T cell responses. Even when antibodies go down, a strong T cell response is capable of protecting the body and can even cause the antibodies to be released faster if the body is exposed to a pathogen a second time. [link]
Because of the specificity, the ability to give booster shots (like what is done with tetanus, measles, mumps, and rubella vacinnes), and the ability to elicit both antibody and T cell responses vaccines can establish and immunity that a disease never will. Additionally a vaccine can target multiple parts of a pathogen so that it will take multiple mutations at the same time to fully escape the immune response.
There’s still hope that we’ll be back to normal one day,
–Your friendly neighborhood scientist
